
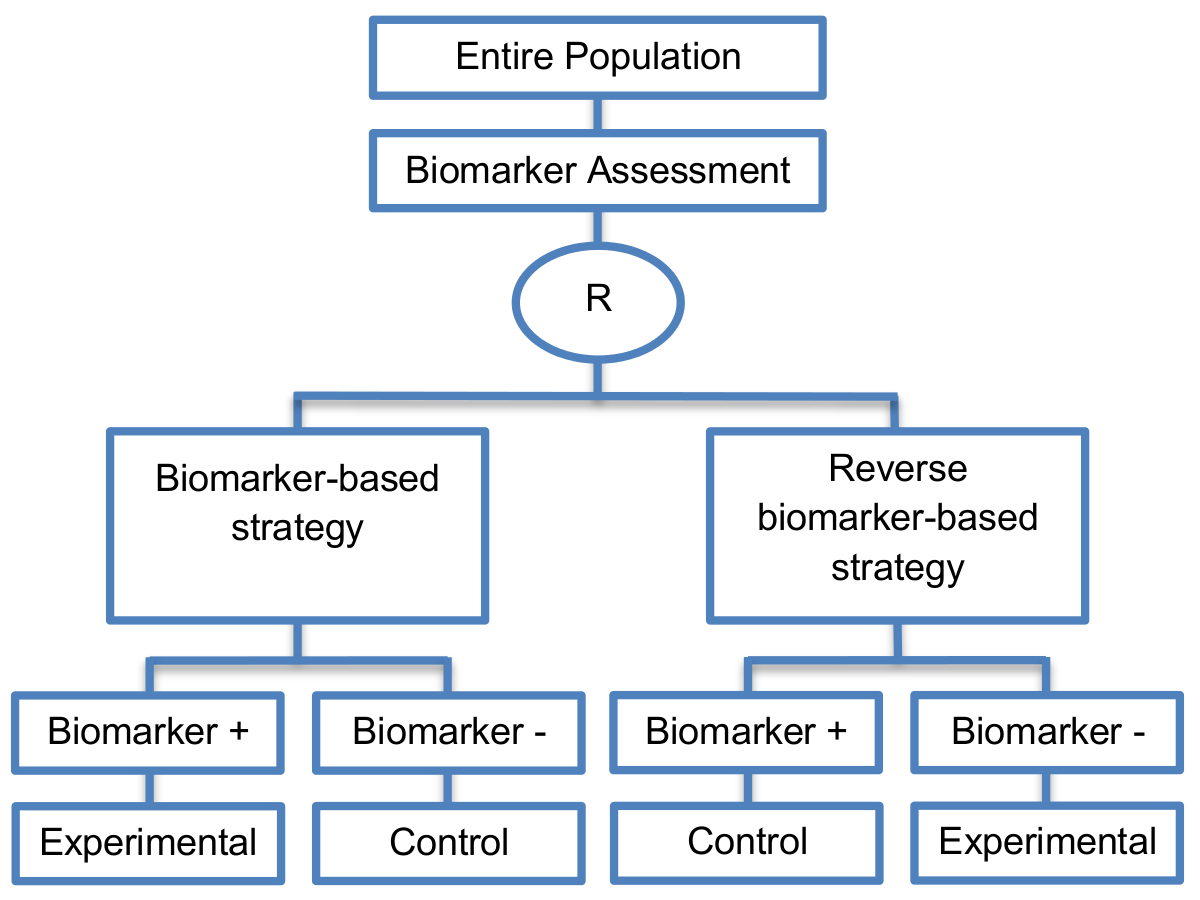
The non-biomarker-based strategy arm which is included in the three subtypes of biomarker-strategy designs is replaced by the reverse marker-strategy arm.
Alternative names: None found
Details
Utility
Reverse marker-based strategy is a more efficient strategy as compared to the first and third biomarker-strategy subtype designs for testing the interaction hypothesis of treatment and biomarker.
Methodology
- These designs should be used in cases where prior evidence indicates that both experimental and control treatment are effective in treating patients but the optimal strategy has not yet been identified.
Sample size Formula
-

 is referred to the
required total number of patients per arm (binary outcome),
is referred to the
required total number of patients per arm (binary outcome),
 is the expected response
rate in the reverse biomarker-based strategy arm and
is the expected response
rate in the reverse biomarker-based strategy arm and
 ,
the expected response rate
,
the expected response rate
 can
be found by calculating the formula
can
be found by calculating the formula
 ,
,
 are the assumed response rates of
biomarker-positive patients receiving the control
treatment and biomarker-negative patients receiving the experimental treatment.
are the assumed response rates of
biomarker-positive patients receiving the control
treatment and biomarker-negative patients receiving the experimental treatment.
Statistical/Practical considerations
Advantages
- Can estimate directly the marker-strategy response rate.
- Allows the estimation of the effect size of the experimental treatment compared to the control treatment for each biomarker-defined subgroup separately.
- There is no chance that the same treatment will be tailored to biomarker-positive patients who are randomized either to the biomarker-based strategy arm or the reverse marker strategy. Also, there is no possibility of the same treatment assignment to biomarker-negative patients who are randomly assigned to the two biomarker-based strategy arms.
- It has been demonstrated by Eng, 2014 [Google Scholar] that these new types of designs are more than four times more efficient for testing the interaction between treatment and biomarker compared to Biomarker-strategy designs with biomarker assessment in the control arm, Biomarker-strategy designs with randomization in the control arm and the marker stratified designs.
Limitations
- It has been claimed by Baker, 2014 [Google Scholar] that other designs than the reverse marker-based strategy are more appropriate in order to investigate questions which include both treatment effect of biomarker-defined subgroups and the biomarker strategy treatment effect. These designs should allow the estimation of treatment effects within biomarker-defined subgroups as well as the estimation of the global treatment effect.
Key references
- Ondra, T.; Dmitrienko, A.; Friede, T.; Graf, A.; Miller, F.; Stallard, N.; Posch, M. Methods for identification and confirmation of targeted subgroups in clinical trials: A systematic review. J. Biopharm. Stat. 2016, 26, 99–119. [Google Scholar] [CrossRef] [PubMed]
- Eng, K.H. Randomized reverse marker strategy design for prospective biomarker validation. Stat. Med. 2014, 33, 3089–3099. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.G. Biomarker evaluation in randomized trials: Addressing different research questions. Stat. Med. 2014, 33, 4139–4140. [Google Scholar] [CrossRef] [PubMed]
- Tanniou, J.; van der Tweel, I.; Teerenstra, S.; Roes, K.C.B. Subgroup analyses in confirmatory clinical trials: Time to be specific about their purposes. BMC Med. Res. Methodol. 2016, 16, 20. [Google Scholar] [CrossRef] [PubMed]
